
When a Life-Saving Drug Exists—but Remains Out of Reach
Imagine knowing that a medicine capable of dramatically extending your child’s life already exists. It has transformed the prognosis of patients in some of the world’s wealthiest countries. Doctors call it revolutionary. Medical journals celebrate it as one of the greatest breakthroughs in the treatment of a rare genetic disease in decades.
Yet, despite all that promise, it remains effectively inaccessible—not because science has failed, but because the price tag is simply too high.
For thousands of families living with cystic fibrosis (CF), this has been reality.
For years, the drug known as Trikafta in the United States and Kaftrio in Europe has represented hope. Instead of merely treating symptoms, it targets the underlying genetic defect responsible for cystic fibrosis, allowing many patients to breathe easier, avoid repeated hospitalizations, and live significantly longer lives. It has fundamentally changed expectations for people born with a disease that once claimed many lives before adulthood.
But there has always been a painful contradiction.
The medicine existed.
The patients existed.
Yet millions of dollars in scientific innovation translated into a treatment that much of the world simply could not afford.
In the United States, the list price of Trikafta is approximately US$370,000 per patient per year, making it one of the most expensive medicines in the world. Patent protections have further prevented generic manufacturers from producing affordable alternatives in many countries. As a result, while children in wealthier nations increasingly gained access to a near-miraculous therapy, thousands elsewhere continued to wait—or never received treatment at all.
Then, unexpectedly, a Bangladeshi pharmaceutical company entered the conversation.
A Small Country Makes a Global Statement
In June 2026, Beximco Pharmaceuticals officially handed over the first supplies of Triko, a generic version of the same three-drug combination therapy that powers Trikafta. The recipients came not only from Bangladesh but from several countries, highlighting that the initiative was never intended to be merely a domestic pharmaceutical launch. It was conceived as a global access project.
The price difference immediately attracted worldwide attention.
Instead of roughly US$370,000 annually, Triko is priced at around US$12,750 per year for adults and US$6,375 for children—about a 96% reduction compared with the branded medicine’s U.S. list price. Campaigners estimate that, at these prices, the cost of treating one child with the branded medicine could instead provide treatment for dozens of children using the generic version.
The announcement was celebrated not only by patients but also by advocacy groups that had spent years campaigning for wider access to cystic fibrosis medicines. For many families, the discussion changed almost overnight from “This medicine is impossible to obtain” to “Perhaps we can finally afford it.”
That is an extraordinary shift.
But to appreciate why this moment matters, we first need to understand what cystic fibrosis actually is—and why Trikafta changed medicine in the first place.
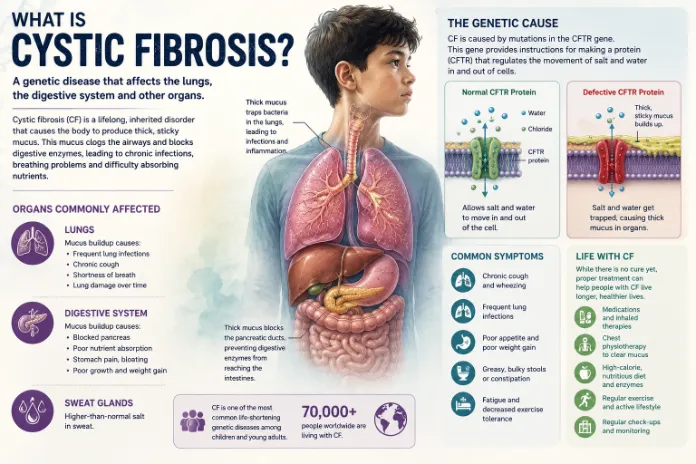
What Is Cystic Fibrosis?
Cystic fibrosis is a rare inherited disease caused by mutations in the CFTR gene. The mutation disrupts the movement of salt and water across cells, producing unusually thick, sticky mucus throughout the body.
The lungs are hit hardest.
Instead of flowing normally, mucus accumulates inside the airways, making breathing progressively more difficult and creating an ideal environment for repeated bacterial infections. Patients often endure chronic coughing, lung damage, and frequent hospital admissions.
The disease affects much more than the lungs.
The same thick secretions can block the pancreas, preventing digestive enzymes from reaching the intestines. Many children struggle to absorb nutrients properly despite eating enough food. Poor growth, malnutrition, vitamin deficiencies, and digestive complications are common.
For decades, treatment focused primarily on managing these consequences rather than correcting the underlying cause.
Doctors prescribed antibiotics to fight infections.
Physiotherapy helped clear mucus.
Digestive enzyme supplements improved nutrition.
These interventions extended life, but they did not fix the faulty protein responsible for the disease itself.
That changed with the arrival of CFTR modulators.
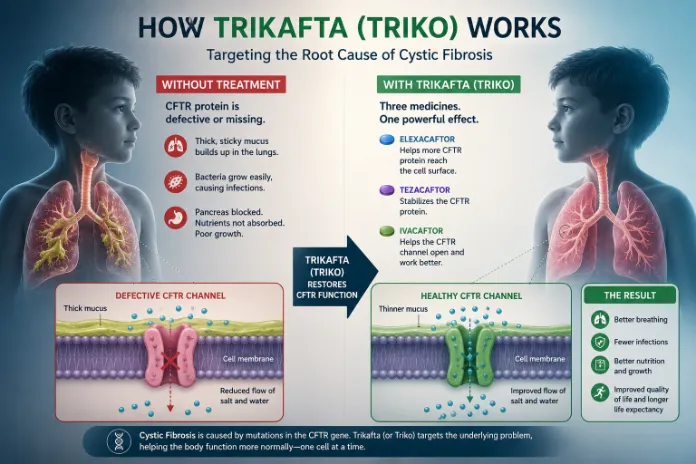
The Drug That Changed Everything
Unlike previous therapies, Trikafta works on the defective CFTR protein itself.
The medicine combines three active ingredients—elexacaftor, tezacaftor, and ivacaftor—that help the faulty protein fold correctly, reach the surface of cells, and function more effectively.
The results have been remarkable.
Many patients experience better lung function within weeks. Hospital admissions often decrease. Respiratory infections become less frequent. Weight gain improves. Quality of life increases substantially.
For many clinicians, Trikafta did not merely represent another new medicine. It redefined what living with cystic fibrosis could look like.
Medical experts frequently describe it as one of the most significant advances in cystic fibrosis treatment in decades because it treats the disease at its biological source rather than only addressing its symptoms.
Yet the greatest obstacle to this breakthrough was never its science.
It was its price.





